Key Takeaways:
- Heart auscultation is part of the cardiac physical exam and involves listening carefully to a patient's heart sounds for the presence of murmurs or rubs.
- Heart sounds are brief sounds produced by the opening and closing of valves. A murmur results from turbulent blood flow. Most murmurs indicate disease, but some are benign. A palpable thrill indicates a severe murmur.
- The hardest part of learning heart auscultation is often learning how to differentiate between all of the heart sounds and murmurs. Being able to correctly analyze what you hear is extraordinarily important and satisfying.
- To learn heart auscultation efficiently and effectively, you should listen to heart sound recordings while observing image and graph animations showing how it all fits together—MedStudy's Heart Sounds can help you do this. This will create an event in your memory, making it easier to remember what function is causing that heart sound or murmur.
- Cardiac exam skills don't improve, on average, after your 3rd year of med school—in most cases, they actually decline.
Before entering clinical rotations, you should learn where to place your stethoscope in order to listen for specific heart sounds and understand how to analyze those sounds. Your attending might call you out to listen to a patient’s heart sound and give your analysis of what's happening—which, depending on your prep, can be a very fun or a very intimidating situation!
Now that you know the challenges you might face with learning heart sounds—and how to avoid those challenges—let’s go through some basics about heart auscultation.
What is heart auscultation?
Heart auscultation is part of the cardiac physical exam and involves listening carefully for the different heart sounds and for the presence of murmurs or rubs. Specific sounds are heard best at different locations over the chest, axilla, or back or with the patient in different positions.
The cardiac physical exam relies on the physician’s senses of sight, hearing, and touch. For example, visual assessment of jugular venous pulsations, auscultation of the heart and lungs, and palpation for thrills and pulses.
The hardest part of learning heart auscultation is often learning to differentiate between all of the heart sounds and murmurs. So, how are successful med students learning heart auscultation? Let’s dive in.
Heart sound locations
Cardiac landmarks are the locations where the stethoscope is placed in order to best listen to each of a patient’s heart sounds. The 4 main landmarks are the RUSB (aortic valve, LUSB (pulmonic valve), LLSB (tricuspid) and the apex (mitral). Note that these locations are not necessarily directly over the valves, but are the best position to hear the valves given the blood flow and surrounding skeletal barriers.
The diaphragm side of the stethoscope filters out low frequency sound and is used to hear high-pitched S1-S4 sounds as well as clicks, snaps, and knocks. It is held with firm pressure that indents the skin a little. Use the bell to listen to low-pitched murmurs and rubs—it works best with just the weight of the stethoscope, so hold it lightly against the skin.
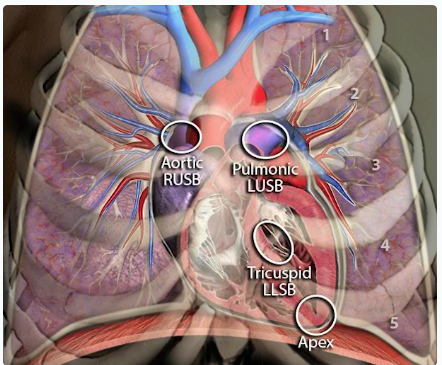
These are the main intercostal cardiac landmarks for stethoscope placement.
Source: MedStudy Heart Sounds
What are the 4 heart sounds?
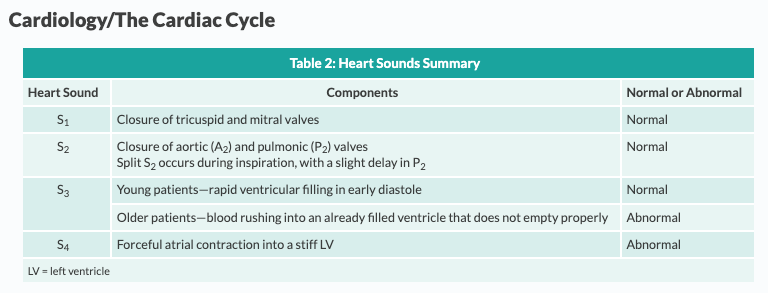
Heart sounds are brief sounds produced by the opening and closing of valves. Systolic heart sounds include the 1st heart sound (S1) and clicks. Diastolic heart sounds include the 2nd, 3rd, and 4th heart sounds (S2, S3, and S4), as well as knocks and snaps.
S1 Heart Sound
S1 is a high-pitched sound caused by the closing of the mitral and tricuspid valves just after the beginning of systole. Mitral valve closure occurs first and is the louder component of S1… (Keep reading)
S2 Heart Sound
S2 is a low-pitched sound caused by the closing of the aortic (A2) and pulmonic (P2) valves at the beginning of diastole. A2 usually occurs just before P2. This physiologic split is larger during inspiration because the increased volume of blood in the RV prolongs RV systole and delays closure of the pulmonic valve. There are several abnormal forms of S2 splitting… (Keep reading)
S3 Heart Sound
S3 is an abnormal heart sound in adults. When present, it occurs in early diastole, immediately after S2. It indicates the end of rapid ventricular filling. On auscultation it creates a pattern that sounds like “Ken-tuck-y,” corresponding to S1, S2, then S3. This often is referred to as a “gallop,” a term coined in 1847 to describe the cadence of 3 heart sounds occurring in rapid succession. The sound is thought to be due to the tensing of the chordae tendineae. S3 often is a normal finding in pregnant women and young children. Otherwise, in adults it usually indicates severe LV systolic dysfunction, especially conditions that increase early LV filling, such as acute ventricular failure or severe aortic or mitral regurgitation. An S3 in a patient with LV dysfunction is a poor prognostic indicator. Note that S3 is best heard during expiration (so that the heart will be closer to the chest wall), using the bell of the stethoscope with the patient in the left lateral decubitus position (i.e., the patient is lying on his left side). (Keep reading)
S4 Heart Sound
S4 is an abnormal heart sound. When present, it occurs just before S1 at the end of diastole. On auscultation, it sounds like “Tenn-e-ssee,” corresponding to S4, S1, and S2, also referred to as a “gallop.” S4 is caused by increased ventricular filling during atrial contraction, occurring in patients with decreased ventricular compliance. You may hear an S4 in ischemic heart disease, AS, HCM, diabetic cardiomyopathy, and hypertensive heart disease with concentric hypertrophy. Note that S4 sometimes occurs with S3 in patients with LV systolic dysfunction but that S4 alone indicates LV diastolic dysfunction. Note that like S3, S4 is best heard using the bell of the stethoscope with the patient in the left lateral decubitus position. (Keep reading)
Other heart sounds
Clicks occur only during systole and are single or multiple. They are briefer and have a higher pitch than S1 or S2. In MVP, a click occurs in mid to late systole and is thought to be due to abnormal tension on the valve leaflets or chordae tendineae. A diastolic knock is a loud, high-pitched, thudding sound that occurs at the same time as S3. It indicates the sudden cessation of rapid ventricular filling due to the presence of a noncompliant pericardium, as in constrictive pericarditis. An opening snap is a brief, high-pitched sound heard best with the diaphragm of the stethoscope at the left lower sternal border (LLSB). It most commonly occurs in early diastole in MS. (Keep reading)
Heart Murmurs
A murmur results from turbulent blood flow. The sound of a murmur is more prolonged than that of the heart sounds. Most murmurs indicate disease, but some are benign. More severe murmurs have thrills, which are palpable vibrations.
There are 3 main descriptors for heart murmurs:
- Timing (i.e., systolic, diastolic, continuous): when the murmur occurs within the cardiac cycle
- Intensity (on a scale of 1–6)
- Location (i.e., where the murmur is heard best):
- Aortic = 2nd right intercostal space
- Pulmonic = 2nd left intercostal space
- Tricuspid = 4th left intercostal space, LLSB
- Mitral = 5th left midclavicular intercostal space (apex of the heart) All murmurs increase in intensity when blood flow increases across the valve.
Memorizing which murmurs are systolic and which are diastolic is important so that you can quickly synthesize a differential diagnosis at the bedside for a patient’s presentation.
The Big Four Heart Murmurs
MedStudy’s Heart Sounds has tips for learning the “Big Four” heart murmurs—Aortic Stenosis, Aortic Regurgitation, Mitral Regurgitation, and Mitral Stenosis—including the timing (systolic, diastolic), intensity, and location where the murmur is heard best.
Diastolic versus systolic murmurs
The cardiac cycle is a sequence of events that occur from one heartbeat to the next. These events begin when an electrical impulse forms at the SA node. As the electrical impulse is conducted through the myocardium, the cardiomyocytes undergo depolarization and repolarization, resulting in contraction and relaxation. This leads to pressure changes that drive blood through the heart and cause valves to open and close. When the valves open and close, they create acoustic vibrations audible as heart sounds.
The cardiac cycle is composed of 2 phases:
- Systole: the ejection phase (ventricular contraction)
- Diastole: the filling phase (ventricular relaxation)
|
Systolic |
Diastolic |
|
Aortic Stenosis Mitral Regurgitation Pulmonic Stenosis Tricuspid Regurgitation |
Aortic Regurgitation Mitral Stenosis Pulmonic Regurgitation Tricuspid Stenosis |
How to study heart sounds
We know one of the best ways to learn—and make information stick in your long-term memory—is to use multiple modalities when learning. Not only should you listen to heart sound recordings, but you should pair what you’re hearing with visually watching what the heart is doing when it makes that sound. This multimodal process will lay down as an "event" (see StudyWise) in your memory, making it easy to remember what function is causing that heart sound or murmur.
In med school? Build your confidence before clinical rotations
Getting questions on a patient's heart sounds during rotations can really put you on the spot. We hope this blog helped break down some of the information! To take it a step further, check out MedStudy Heart Sounds. This resource will teach you to accurately identify what you’re hearing and seeing when you assess a patient.
MedStudy Heart Sounds is an interactive experience covering cardiac anatomy, blood flow, the cardiac cycle (with animated Wiggers diagram), neck pulsations, and the big four heart murmurs. It even gives you real clinical scenarios and a heart sounds quiz to test your knowledge. Per feedback, we know MedStudy Heart Sounds has helped thousands of residents and physicians learn heart auscultation more efficiently and effectively (and it's likely being used by the standout med students in your class!). You can try it and see for yourself by signing up for a 24-hour free trial.
You can build on your cardiology knowledge even more with the Core Cardiology book—it breaks down the Cardiology topics covered in med school classwork and on USMLE and COMLEX exams into casual, concise written and visual “lectures."