It's Nutrition Month! Brush up with this section from our Pediatrics Core on the 6 nutritional disorders you'll need to know for boards and patient care.
Start with the MedStudy Method
Preview | Review Questions
Have you heard about the Preview | Review Questions at the beginning of each section in our Pediatrics Core? These questions help you prime your brain and dredge up what you know about the topic you're studying. Look out for the green box at the beginning of each new section for relevant questions. Use P|R Questions to preview, study, and review the highest-yield material.
Highlighted Text
As you read the text, the highlighted areas will give you the answers to the Preview | Review Questions.
So, first, preview the material. Read through the questions on Nutritional Disorders and dredge up all the info you can in your head about it.
Later on, you'll study. Read through the text, paying extra attention to the highlighted areas. The highlighted text includes must-know concepts and the answers to the Preview | Review Questions. The work you did previewing the material should have made your brain sticky to retain this information.
Preview | Review section on Nutritional Disorders from the Pediatrics Core
You'll then enter the spaced retrieval stage which focuses on self-testing. Use the Preview | Review questions like Q&As. Then, go through the highlighted text to find the answers, plus any other nuggets of information you should know before the exam. If you have set up your Personal Trainer, it will set this up for you.
6 nutritional disorders you need to know as a pediatrician
Now that we've gone over how to study, let's dive into the review.
1. MARASMUS

Marasmus Source: CDC/Dr. Edward Brink
Severe calorie malnutrition in a child is called marasmus. The term “marasmus” is being phased out by some and replaced with the term “protein-energy malnutrition without edema.”
These children have generalized loss of muscle and no subcutaneous fat. They appear to be emaciated and cachectic. Linear growth is also affected if the malnutrition persists long enough. These patients have very loose, wrinkled skin because of the loss of the subcutaneous fat. The face is described as looking like a “wizened old man” due to the loss of temporal and buccal fat pads. Note that buccal fat pads are the last to go; their loss is a sign of long-lasting, severe malnutrition.
Affected children frequently are hypothermic, bradycardic, and hypotensive; these conditions result from the body’s adaptation to the prolonged duration of inadequate energy stores.
2. KWASHIORKOR

Kwashiorkor Source: CDC/Dr. Lyle Conrad
Insufficient intake of protein causes kwashiorkor. It is frequently associated with an inadequate intake of calories, but not in all cases. Kwashiorkor is a Ghanaian term that means “the disease of the deposed baby when the next one is born.” The term “kwashiorkor” is also being phased out by some and replaced with “protein-energy malnutrition with edema.”
Typically, kwashiorkor appears in young children during or just after the weaning process. Kwashiorkor is epidemic in developing countries because the main calorie sources in these regions are carbohydrates that are low in protein—particularly white rice, cassava, and yams. Those affected are sometimes called “sugar babies.” This type of malnutrition can make a child appear “fat,” but this swelling is primarily edema, caused by hypoalbuminemia and resultant low oncotic pressure.
In affected children, the extent of malnutrition may be masked by the edema, which is typically soft, pitting, and painless, usually involving the feet and legs. In severe cases, it can extend to the face and upper extremities. Most affected children have skin rashes that can include hyperkeratosis and pigmentation changes due to desquamation of the epidermis. The rash has sharply demarcated edges with a reddish-brown, scaly surface overlying blanching erythema. The hair is dry and brittle and becomes yellowish-gray. In children who have fluctuating nutrition (some months good, other months poor), a “flag sign” may develop, which refers to areas of normal hair alternating with areas of depigmentation.
Children with kwashiorkor usually have livers enlarged by fatty infiltration. T-cell function and cell-mediated immunity are abnormal in these children, and they are at increased risk for infection.
While the classic distinction between marasmus and kwashiorkor has been taught for decades (marasmus = severe nutritional and caloric deficiency in general; kwashiorkor = protein deficiency), the actual mechanism of malnutrition is more complex. A combination of impaired immunity, chronic bacterial GI infection, and malnutrition are likely to blame. The line between marasmus and kwashiorkor is often blurred.
3. ETIOLOGY-BASED MALNUTRITION
Marasmus and kwashiorkor are rarely seen in developed countries. Instead, malnutrition is seen in the context of an underlying disease process. Malnutrition is defined by etiology—either by illness or nonillness (caused by environmental or behavioral factors). The parameters to define malnutrition are based on anthropometric Z-scores, which are the number of standard deviations from the means of the growth curves. Acute is defined as < 3 months in duration and chronic as longer. A body mass index (BMI) Z-score of < –1.0 to –2.0 is mild; –2.0 to –3.0 is moderate; and > –3.0 is severe. Once the diagnosis of malnutrition is made, the underlying cause for it must be found. For instance, a child with congenital heart disease and a BMI Z-score of –2.3 has moderate chronic malnutrition due to congenital heart disease.
4. FAT-SOLUBLE VITAMIN DEFICIENCIES
Vitamins A, D, E, and K are fat-soluble vitamins and require carrier proteins for transport. Adequate uptake of these nutrients requires intact mechanisms for fat digestion and absorption. Inadequate liver (bile salts for micelle formation) and pancreatic (lipases) function are the most common sources of diseases affecting fat digestion. Diseases that result in pancreatic insufficiency (e.g., cystic fibrosis) can utilize oral replacement enzymes to prevent malabsorption of the fat-soluble vitamins. Vitamins A and D are transported by specific plasma proteins, and vitamins E and K are transported mostly by low-density lipoproteins (LDLs). All of these vitamins are responsible for regulating protein synthesis. Know the complications caused by these vitamin deficiencies. You can read more about Vitamin A, D, E, and K deficiencies in the Nutritional Disorders section of the Pediatrics Core.
5. WATER-SOLUBLE VITAMIN DEFICIENCIES
Vitamin C Deficiency (Scurvy)
Vitamin C (ascorbic acid) deficiency, a.k.a. scurvy, is rare in developed countries. Dietary sources include citrus fruits, tomatoes, potatoes, strawberries, cauliflower, broccoli, Brussels sprouts, and spinach. Vitamin C deficiency mostly occurs in children between 6 months and 2 years of age. It can also be seen in the homeless and in individuals who use drugs and/or misuse alcohol. Initial symptoms are nonspecific and include irritability, digestive disturbances, and anorexia. Classic physical descriptions include follicular hyperkeratosis, perifollicular hemorrhages, and “corkscrew-coiled” hairs. The skin commonly has petechiae and purpura, and gingival bleeding is also common. Normochromic, normocytic anemia is found in ~ 75% of patients with scurvy. Joint complaints can occur due to hemarthrosis.
Vitamin C deficiency results in impaired formation of collagen and chondroitin sulfate. The lack of collagen results in fragile capillaries and gingival hemorrhage; the lack of chondroitin sulfate results in failed osteoid formation by osteoblasts, causing the cessation of endochondral bone formation. In other words, bones become brittle and fracture easily. Most of the abnormalities are found at the metaphyseal zone of tubular bones and at the sternal-rib junctions.
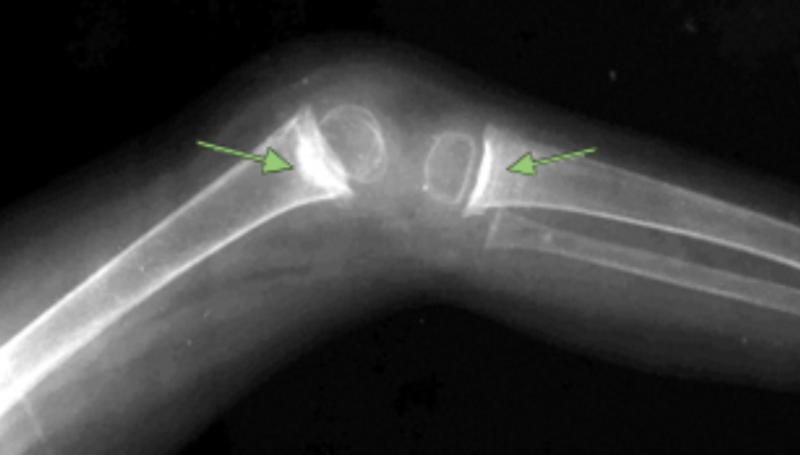
One of the important x-ray findings in scurvy are the white lines of Frankel: a dense band at the growing metaphyseal end, involving the provisional zone of calcification.

White lines of Frankel with a patient with vitamin C deficiency
Treat vitamin C deficiency with oral ascorbic acid.
Read about more water-soluble vitamin deficiencies in the Pediatrics Core.
6. PICA
The repeated oral ingestion of nonfood items (such as dirt, paper, hair, and rocks) for at least 1 month characterizes pica. It is inappropriate for the developmental level of the child. Pica is classically associated with iron deficiency and lead exposure, so remember to check for these in a child with pica. It is most common in individuals between 2 and 3 years of age and in those with developmental disabilities. Although pica often eventually remits spontaneously, careful monitoring is necessary due to the risk of medical complications. These include lead poisoning (ask about the age of the house and the presence of paint chips!), parasitic infections, and GI obstruction. Pica can also lead to deficiencies in iron, Ca2+, zinc, and other nutrients (e.g., thiamin, niacin, vitamins C and D).
Like the way these points are high-yield and only what you need to know for the ABP Boards? Get the full Pediatrics Core to fully utilize the Preview | Review Questions, highlighted areas, and much more content!
Want more info on The MedStudy Method? Check out our StudyWise guide.